About the project
Check out our progress
The initial research phase focused on understanding the challenges associated with prostate biopsy procedures and identifying potential technological solutions. This involved a comprehensive review of existing biopsy techniques, imaging modalities, and robotic systems used in medical applications.

Initial ultrasound probe mount protoypes
In order to integrate our system with existing clinical workflows, we analyzed current practices and identified key areas where robotic assistance could enhance precision and reduce patient discomfort. This phase also included consultations with medical professionals to gather insights and validate our approach.

Prostate phantoms used for testing and calibration
Additionally, we explored state-of-the-art AI techniques for medical imaging analysis, focusing on their potential to improve the detection and localization of suspicious prostate regions. This research laid the groundwork for the subsequent development phases of the project.
Overall, the initial research phase was crucial in shaping the direction of our project and establishing a solid foundation for the development of our robotic prostate biopsy system.
Most importantly, we assembled a multidisciplinary team with expertise in robotics, medical imaging, and clinical practice to drive the project forward. We planned for seamless clinical integration by engaging with healthcare professionals early in the process to ensure our solutions align with real-world needs.
Developing precise and reliable control algorithms for the robotic system to ensure accurate needle placement during the biopsy procedure. This includes kinematic modeling, motion planning, and control strategies to achieve the desired performance and safety standards.
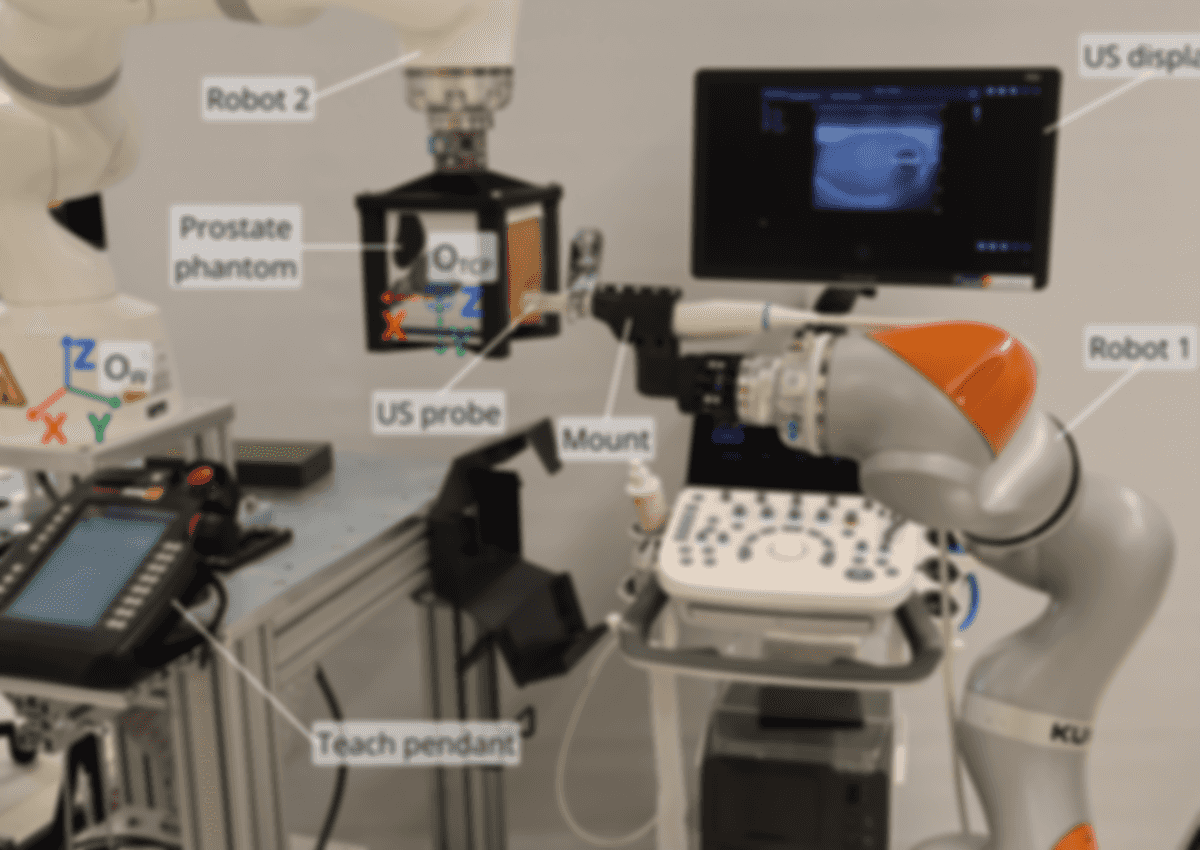
Robot control setup used during test biopsy procedures
A crucial aspect to consider is movement compensation. Since the prostate can shift due to patient movement or physiological factors, the robotic system must be capable of adapting in real-time to these changes. This involves integrating sensors and feedback mechanisms to monitor prostate position and adjust the robot's actions accordingly.
Clinicians contribute valuable insights in this area to ensure that the robotic system can be seamlessly integrated into existing clinical workflows. This includes considerations for ease of use, safety, and compatibility with other medical equipment.
Currently, we use a force sensor and visual servoing to minimize the error caused by prostate motion during the biopsy procedure. This allows the robot to adjust its position in real-time, ensuring accurate needle placement despite any movement of the prostate.
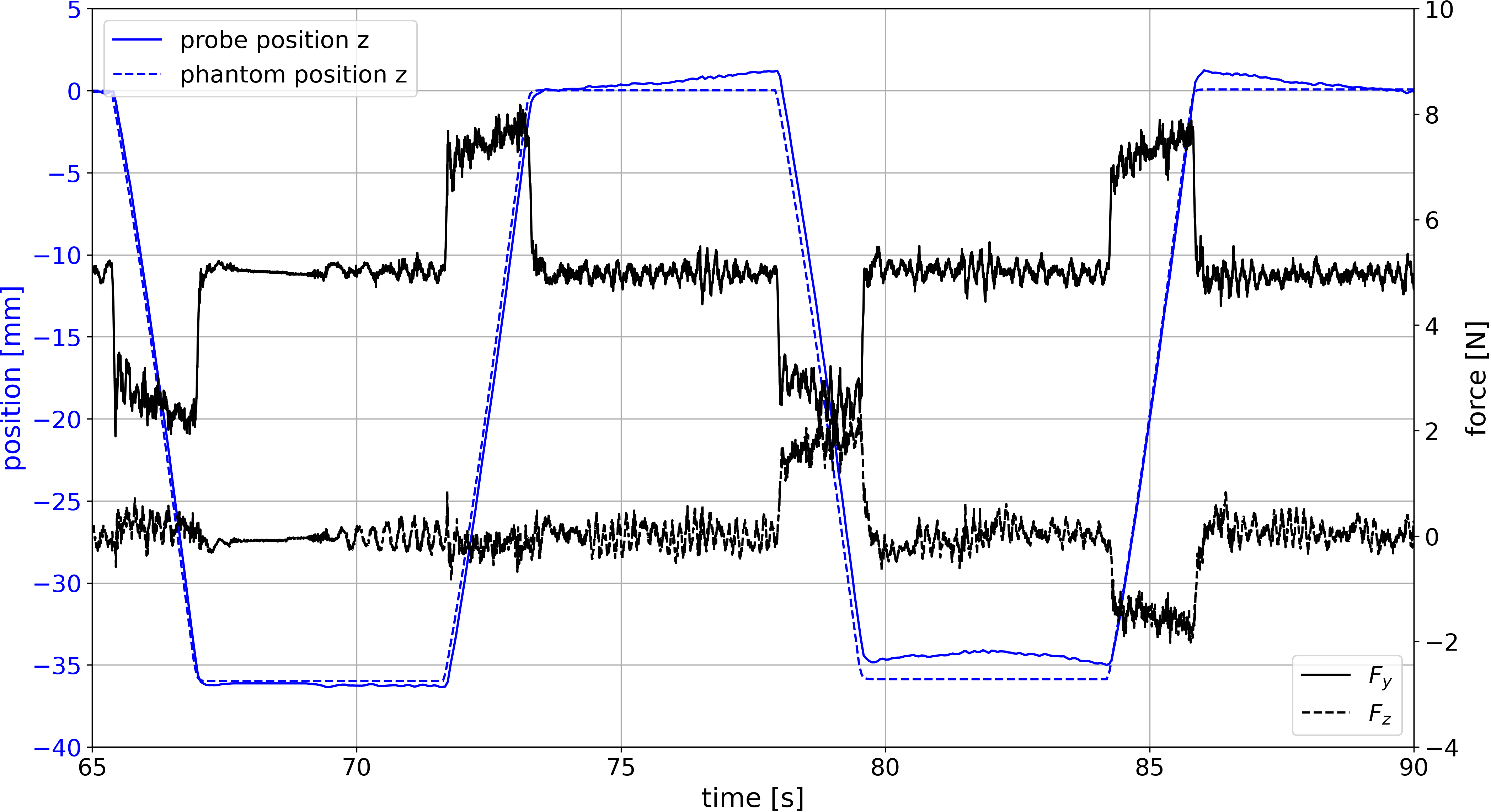
Graph showing vertical motion compensation during test biopsy procedure
Our next step was to optimize robot position to meet the clinician's demands. As they traditionally work with a lowered setup, we lowered the prostate phantom to make our prototype easier to test and more realistic. This also improves the usability of the system in a clinical setting.
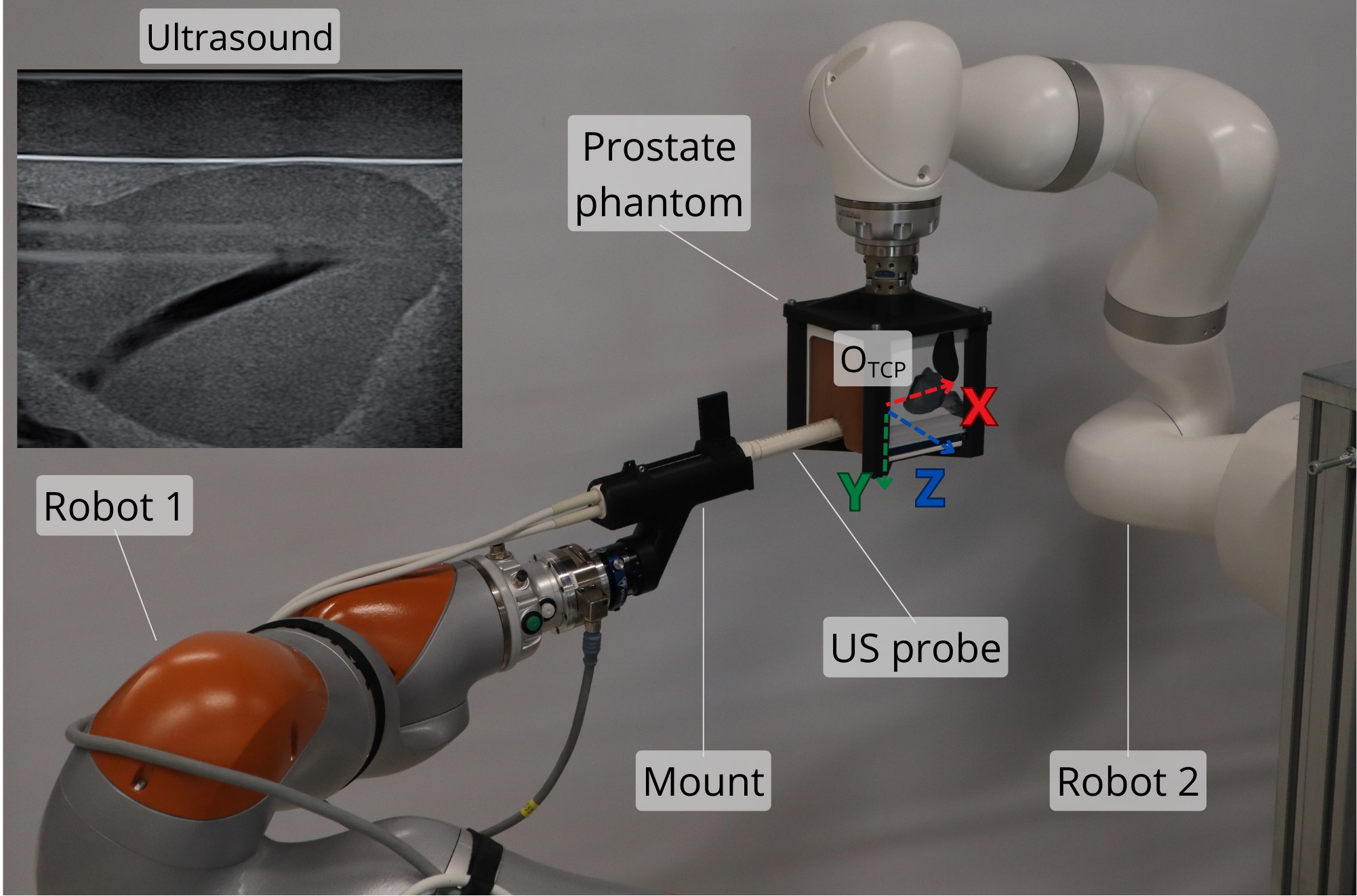
Improved robot setup
High-quality data remains one of the biggest bottlenecks in developing reliable AI models. This is especially true in medical environments, where accuracy, robustness, and trust are essential because clinical decisions directly affect human lives. To help address this challenge, we are building a large, carefully annotated micro-ultrasound imaging dataset.
Working closely with clinicians, our team has labeled gigabytes of imaging data to create a high-quality foundation for training and validating advanced AI models. This enables us to further improve our own segmentation, detection, and decision-support systems for prostate imaging and biopsy planning.
Equally important, we are committed to open-sourcing as much data as possible so that other researchers can use it to develop, compare, and validate their own methods. By making high-quality medical imaging data more accessible, we hope to accelerate innovation, encourage collaboration, and support the development of safer and more effective AI solutions in healthcare.
Datasets
Micro-ultrasound image dataset
Our first dataset consists of approximately 500 GB of micro-ultrasound data. In close collaboration with clinicians, we successfully annotated a large portion of this dataset using our internally developed Medical Annotation Platform (MedAP). This high-quality annotated data provides a strong foundation for developing and validating advanced AI models for medical imaging applications.
We would especially like to thank our colleagues from the School of Medicine, University of Zagreb, whose clinical expertise was essential throughout the annotation process. Their guidance and domain knowledge significantly improved the quality, accuracy, and clinical relevance of the dataset. Without their contribution, the value of this dataset would have been substantially lower.
We hope this dataset is useful to other researchers in developing new models. You can explore our dataset and use it freely under the specified license. Find out more information about the dataset at this link.
Micro-ultrasound biopsy video dataset
Biopsy videos are micro-ultrasound recordings captured during prostate biopsy procedures, where both the prostate anatomy and needle penetration can be clearly observed in real time. These videos contain valuable procedural and imaging information that can support the development of next-generation AI tools for prostate cancer diagnosis and intervention planning.
We are currently organizing and structuring a dedicated video dataset that combines biopsy recordings with accompanying histopathological findings. By linking imaging data with confirmed pathology results, this dataset creates an important foundation for supervised learning approaches aimed at identifying patterns associated with malignant and benign tissue.
Our long-term objective is to develop new AI models for prostate cancer classification that can assist clinicians during biopsy procedures and improve decision-making through real-time image analysis. Such tools could help increase diagnostic accuracy, reduce uncertainty, and support more targeted interventions.
We also aim to open-source this dataset in the future, enabling other researchers to explore new methods, benchmark algorithms, and contribute to progress in medical imaging AI. By making high-quality multimodal datasets more accessible, we hope to encourage collaboration and accelerate innovation in prostate cancer diagnostics.
Traditional biopsy procedure probe trajectory dataset
Our newest endeavor focuses on developing custom ultrasound probe marker mounts and using our Polaris optical tracking system to monitor probe position throughout conventional biopsy procedures. This allows us to capture precise motion and orientation data during real clinical workflows, providing valuable insight into how clinicians manipulate the probe during interventions.
The collected tracking data serves as an important baseline for refining our robotic system parameters, motion strategies, and control algorithms. By studying expert clinical practice, we can better tune our robotic approach to replicate effective probe handling, improve workflow compatibility, and enhance overall procedural accuracy.
With the support of our clinical collaborators, we have already gathered data from more than 30 procedures involving different patients. This growing dataset represents a valuable bridge between traditional clinical expertise and next-generation robotic assistance, helping ensure that our solutions are grounded in real-world medical practice.
Trajectory tracking setup
Integrating advanced imaging techniques such as micro-TRUS and AI algorithms to enhance the detection and localization of suspicious prostate regions. This includes developing machine learning models to analyze imaging data and assist in biopsy planning.
Most importantly, we use AI to segment the prostate and suspicious regions from micro-TRUS images. This allows us to create a detailed 3D model of the prostate, which is essential for accurate biopsy planning and needle guidance. This approach reduces the cognitive load on clinicians and improves the overall accuracy of the biopsy procedure.
Based on the MicroSegNet architecture, we developed a custom neural network tailored for the segmentation of prostate and suspicious regions from micro-TRUS images. This model was trained on a diverse dataset of annotated images to ensure robust performance across various clinical scenarios.

Neural network architecture used for prostate and suspicious region segmentation from micro TRUS images
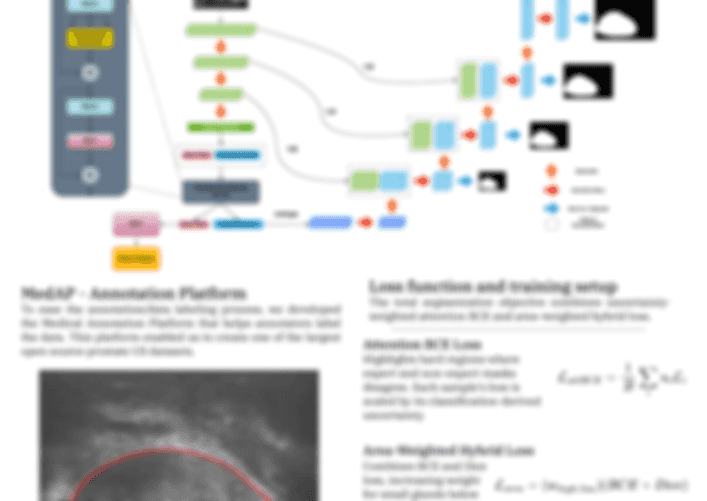
Poster presenting our Neural Network.
